Download Advance Beneficiary Notice of Non-coverage Template
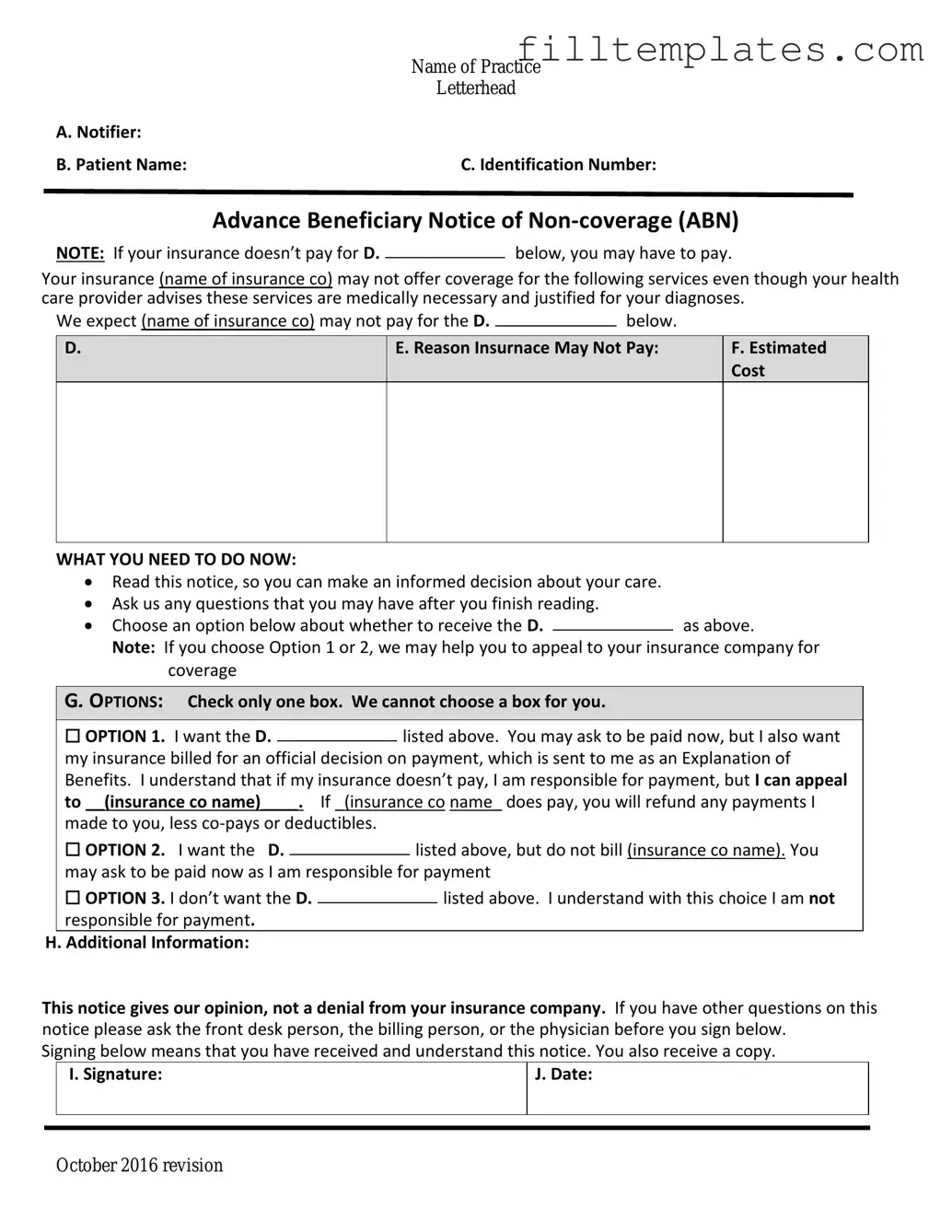
The Advance Beneficiary Notice of Non-coverage, commonly referred to as the ABN, plays a crucial role in the healthcare landscape for Medicare beneficiaries. This form serves as a notification to patients when a healthcare provider believes that a service or item may not be covered by Medicare. By providing this notice, providers help patients understand their financial responsibilities ahead of time, allowing them to make informed decisions about their care. The ABN outlines the specific service in question, the reason why it may not be covered, and the estimated cost to the patient if they choose to proceed. Importantly, the form also offers patients the opportunity to accept or refuse the service, thereby empowering them in their healthcare journey. Understanding the nuances of the ABN is essential for beneficiaries to navigate potential out-of-pocket expenses and ensure they are fully informed about their options. With this knowledge, patients can engage more actively in discussions with their healthcare providers and make choices that align with their health needs and financial situations.
Key takeaways
When dealing with the Advance Beneficiary Notice of Non-coverage (ABN), understanding its purpose and proper usage is crucial for both healthcare providers and patients. Here are key takeaways to consider:
- Purpose of the ABN: The ABN informs patients that a service may not be covered by Medicare. It allows patients to make informed decisions about their care and potential costs.
- Completion Requirements: Providers must fill out the ABN accurately, including the specific service being provided, the reason for non-coverage, and the estimated costs. This ensures transparency and clarity for the patient.
- Patient Signature: Patients should sign the ABN to acknowledge that they understand the potential for non-coverage. This signature is essential for the provider to proceed with the service and for the patient to accept financial responsibility.
- Retention of Records: Providers must keep a copy of the signed ABN in their records. This documentation is important for compliance and may be needed for future reference or audits.
Guide to Writing Advance Beneficiary Notice of Non-coverage
After receiving the Advance Beneficiary Notice of Non-coverage form, you will need to fill it out accurately to ensure proper communication regarding your healthcare services. This form helps clarify your financial responsibilities for services that Medicare may not cover. Follow these steps to complete it correctly.
- Start by entering your personal information at the top of the form. This includes your name, address, and Medicare number.
- Next, provide the date on which you are filling out the form.
- Indicate the specific service or item that you are receiving. Be clear and precise to avoid confusion.
- In the designated section, explain why you believe Medicare should cover the service. Use straightforward language to outline your reasons.
- Review the information you have provided to ensure it is accurate and complete.
- Sign and date the form at the bottom. Your signature confirms that you understand the information presented.
- Make a copy of the completed form for your records before submitting it to the appropriate party.
Browse Other PDFs
Hoa Proxy Form - This form helps maintain a well-functioning and responsive Association.
Cash Receipt Voucher - Key for managing operating expenses through cash inflow.
The Durable Power of Attorney document serves as a critical resource for individuals looking to secure their financial decisions through trusted representation during challenging times. By using this form, you can ensure that your preferences are honored even when you may not be able to communicate them effectively due to health issues.
Can a Therapist Write an Esa Letter - Understanding housing laws regarding ESAs can help individuals navigate potential challenges.
Form Preview Example
|
Name of Practice |
|
Letterhead |
A. Notifier: |
|
B. Patient Name: |
C. Identification Number: |
Advance Beneficiary Notice of
NOTE: If your insurance doesn’t pay for D.below, you may have to pay.
Your insurance (name of insurance co) may not offer coverage for the following services even though your health care provider advises these services are medically necessary and justified for your diagnoses.
We expect (name of insurance co) may not pay for the D. |
|
below. |
|
D.
E. Reason Insurnace May Not Pay:
F.Estimated Cost
WHAT YOU NEED TO DO NOW:
Read this notice, so you can make an informed decision about your care.
Ask us any questions that you may have after you finish reading.
Choose an option below about whether to receive the D.as above.
Note: If you choose Option 1 or 2, we may help you to appeal to your insurance company for coverage
G. OPTIONS: Check only one box. We cannot choose a box for you.
|
☐ OPTION 1. I want the D. |
|
listed above. You may ask to be paid now, but I also want |
||||
|
|
||||||
|
my insurance billed for an official decision on payment, which is sent to me as an Explanation of |
||||||
|
Benefits. I understand that if my insurance doesn’t pay, I am responsible for payment, but I can appeal |
||||||
|
to __(insurance co name)____. If _(insurance co name_ does pay, you will refund any payments I |
||||||
|
made to you, less |
|
|
|
|||
|
☐ OPTION 2. I want the D. |
|
|
listed above, but do not bill (insurance co name). You |
|||
|
|
|
|||||
|
may ask to be paid now as I am responsible for payment |
||||||
|
☐ OPTION 3. I don’t want the D. |
|
|
|
listed above. I understand with this choice I am not |
||
|
|
|
|
||||
|
responsible for payment. |
|
|
|
|||
H. Additional Information: |
|
|
|
||||
This notice gives our opinion, not a denial from your insurance company. If you have other questions on this notice please ask the front desk person, the billing person, or the physician before you sign below.
Signing below means that you have received and understand this notice. You also receive a copy.
|
I. Signature: |
J. Date: |
|
|
|
|
|
|
October 2016 revision
Documents used along the form
The Advance Beneficiary Notice of Non-coverage (ABN) is an important document that informs patients about services that may not be covered by Medicare. Alongside the ABN, several other forms and documents are commonly used to ensure clear communication and understanding regarding healthcare services and coverage. Below is a list of these related documents.
- Medicare Summary Notice (MSN): This document provides beneficiaries with a summary of the services they received, the amount billed, and what Medicare paid. It helps patients understand their financial responsibility.
- Notice of Exclusion from Medicare Benefits (NEMB): This notice informs beneficiaries that a specific service is excluded from Medicare coverage. It details the reasons for the exclusion and any potential out-of-pocket costs.
- Patient Consent Form: This form is used to obtain a patient’s consent before providing specific treatments or services. It ensures that patients are informed about what to expect and agree to the procedures.
- FedEx Bill of Lading Form: This essential document details the terms and conditions of a shipment and is vital for accuracy in processing shipments, as outlined by OnlineLawDocs.com.
- Claim Form: This document is submitted to Medicare or other insurers to request payment for services rendered. It includes details about the patient, the provider, and the services provided.
Understanding these documents helps patients navigate their healthcare options and make informed decisions about their care. Each form plays a crucial role in the communication process between healthcare providers and patients.