Download CDC U.S. Standard Certificate of Live Birth Template
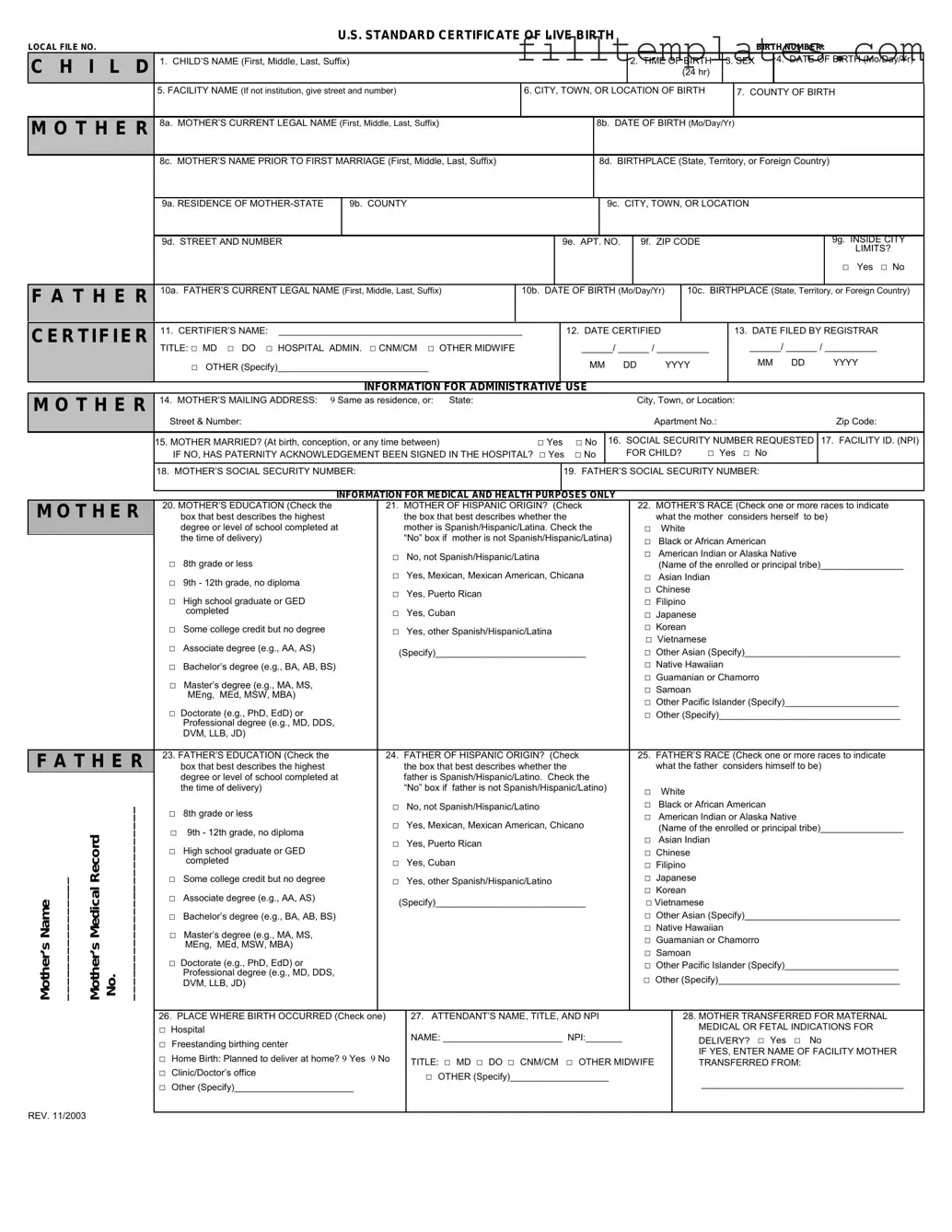
The CDC U.S. Standard Certificate of Live Birth form is an essential document that captures vital information about a newborn. It plays a crucial role in public health, legal identification, and statistical purposes. This form includes key details such as the baby's name, date of birth, and place of birth, along with information about the parents, including their names, birthplaces, and addresses. Additionally, the form collects data on the mother's health during pregnancy, the type of delivery, and any complications that may have occurred. This comprehensive approach ensures that the birth is accurately recorded, which is important for future healthcare and demographic studies. By standardizing the information collected, the form helps maintain consistency across states and facilitates the tracking of health trends over time.
Key takeaways
Filling out the CDC U.S. Standard Certificate of Live Birth form can seem daunting, but understanding its key components can make the process smoother. Here are some essential takeaways to keep in mind:
- Accuracy is Crucial: Ensure that all information is filled out accurately. This includes details like the baby’s name, date of birth, and parent information. Errors can lead to complications later, such as issues with obtaining a Social Security number.
- Gather Necessary Information: Before starting the form, collect all required information. This includes parents’ full names, addresses, and dates of birth. Having everything on hand can speed up the process.
- Signature Requirements: Both parents may need to sign the form, depending on state regulations. Make sure to check local requirements to avoid delays in processing.
- Timeliness Matters: Submit the completed form as soon as possible, ideally within the first few weeks after birth. This helps ensure that the birth is registered in a timely manner, which is important for legal and health records.
By keeping these points in mind, you can navigate the process of filling out the Certificate of Live Birth with confidence and ease.
Guide to Writing CDC U.S. Standard Certificate of Live Birth
Completing the CDC U.S. Standard Certificate of Live Birth form is an essential step in documenting the birth of a child. This form requires accurate information to ensure proper registration and compliance with state regulations. Once the form is filled out, it will need to be submitted to the appropriate state or local vital records office for processing.
- Begin by gathering necessary information. You will need details about the child, parents, and the birth event.
- Fill in the child's full name, including first, middle, and last names.
- Enter the child's date of birth, including the month, day, and year.
- Provide the place of birth, specifying the city, county, and state.
- Indicate the sex of the child by marking the appropriate box.
- Complete the section for the parents' information. This includes full names, addresses, and dates of birth for both parents.
- Fill in the parents' place of birth, specifying the city and state.
- Include the parents' marital status at the time of the child's birth.
- Provide the name of the attending physician or midwife, along with their contact information.
- Sign and date the form at the designated area. Both parents may need to sign, depending on state requirements.
- Review the form for accuracy. Ensure all sections are completed and information is correct.
- Submit the completed form to the appropriate vital records office along with any required fees.
Browse Other PDFs
Bill of Lading Meaning - It is advisable to keep multiple copies of the Bill of Lading.
The Aaa International Driving Permit Application form is essential for U.S. citizens seeking to drive legally in various countries, as it is universally recognized and translates your existing driver’s license. To streamline your travel preparations, consider obtaining the Aaa International Driving Permit Application form, which can greatly enhance your driving experience and offer reassurance while navigating unfamiliar roads.
Lic 603a - Facilities must report any changes in staff to the licensing agency in a timely manner.
Free Printable Puppy Health Guarantee - Only purebred puppies are sold under this agreement.
Form Preview Example

U.S. STANDARD CERTIFICATE OF LIVE BIRTH
LOCAL FILE NO. |
|
|
|
|
|
|
BIRTH NUMBER: |
|
C H I L D |
1. CHILD’S NAME (First, Middle, Last, Suffix) |
|
|
2. TIME OF BIRTH |
3. SEX |
|
4. DATE OF BIRTH (Mo/Day/Yr) |
|
|
|
|
(24 hr) |
|
|
|
|
|
|
5. FACILITY NAME (If not institution, give street and number) |
6. CITY, TOWN, OR LOCATION OF BIRTH |
|
7. COUNTY OF BIRTH |
||||
|
|
|
8b. DATE OF BIRTH (Mo/Day/Yr) |
|
|
|
||
M O T H E R |
8a. MOTHER’S CURRENT LEGAL NAME (First, Middle, Last, Suffix) |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
8c. MOTHER’S NAME PRIOR TO FIRST MARRIAGE (First, Middle, Last, Suffix)
8d. BIRTHPLACE (State, Territory, or Foreign Country)
|
9a. RESIDENCE OF |
|
9b. COUNTY |
|
|
|
|
|
9c. CITY, TOWN, OR LOCATION |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
9d. STREET AND NUMBER |
|
|
|
|
9e. APT. |
NO. |
|
9f. ZIP CODE |
|
|
|
|
9g. INSIDE CITY |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LIMITS? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
□ Yes □ No |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
F A T H E R |
10a. FATHER’S CURRENT LEGAL NAME (First, Middle, Last, Suffix) |
10b. DATE OF BIRTH (Mo/Day/Yr) |
|
10c. BIRTHPLACE (State, Territory, or Foreign Country) |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||
CERTIFIER |
11. CERTIFIER’S NAME: _______________________________________________ |
|
12. DATE CERTIFIED |
|
|
|
13. DATE FILED BY REGISTRAR |
|||||||||||
|
TITLE: □ MD □ DO □ HOSPITAL ADMIN. □ CNM/CM □ OTHER MIDWIFE |
|
|
|
______/ ______ / __________ |
|
______/ ______ / __________ |
|||||||||||
|
□ OTHER (Specify)_____________________________ |
|
|
|
MM |
DD |
YYYY |
|
|
MM DD |
|
YYYY |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
INFORMATION FOR ADMINISTRATIVE |
USE |
|
|
|
|
|
|
|
|
|
|||||
M O T H E R |
14. MOTHER’S MAILING ADDRESS: |
9 Same as residence, or: State: |
|
|
|
|
|
|
|
City, Town, or Location: |
|
|
|
|||||
|
Street & Number: |
|
|
|
|
|
|
|
|
|
Apartment No.: |
|
|
Zip Code: |
||||
|
15. MOTHER MARRIED? (At birth, conception, or any time between) |
□ Yes |
□ No |
16. SOCIAL SECURITY NUMBER REQUESTED |
17. FACILITY ID. (NPI) |
|||||||||||||
|
IF NO, HAS PATERNITY ACKNOWLEDGEMENT BEEN SIGNED IN THE HOSPITAL? □ Yes |
□ No |
|
FOR CHILD? |
□ Yes |
□ No |
|
|
||||||||||
|
18. MOTHER’S SOCIAL SECURITY NUMBER: |
|
|
19. FATHER’S SOCIAL SECURITY NUMBER: |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
INFORMATION FOR MEDICAL AND HEALTH PURPOSES ONLY |
|
|
|
|
|
|
|
|
|
|||||||
M O T H E R
F A T H E R
Mother’s Name ________________ |
Mother’s Medical Record No. _________________________ |
20. MOTHER’S EDUCATION (Check the |
21. MOTHER OF HISPANIC ORIGIN? (Check |
|||
|
box that best describes the highest |
|
the box that best describes whether the |
|
|
degree or level of school completed at |
|
mother is Spanish/Hispanic/Latina. Check the |
|
|
the time of delivery) |
|
“No” box if mother is not Spanish/Hispanic/Latina) |
|
□ |
8th grade or less |
□ |
No, not Spanish/Hispanic/Latina |
|
□ Yes, Mexican, Mexican American, Chicana |
||||
□ |
9th - 12th grade, no diploma |
|||
□ |
Yes, Puerto Rican |
|||
□ |
High school graduate or GED |
|||
□ |
|
|||
|
completed |
Yes, Cuban |
||
□ |
Some college credit but no degree |
□ |
Yes, other Spanish/Hispanic/Latina |
|
□ Associate degree (e.g., AA, AS) |
|
(Specify)_____________________________ |
||
|
|
|
||
□Bachelor’s degree (e.g., BA, AB, BS)
□Master’s degree (e.g., MA, MS, MEng, MEd, MSW, MBA)
□Doctorate (e.g., PhD, EdD) or Professional degree (e.g., MD, DDS, DVM, LLB, JD)
23. FATHER’S EDUCATION (Check the |
24. FATHER OF HISPANIC ORIGIN? (Check |
|||
|
box that best describes the highest |
|
the box that best describes whether the |
|
|
degree or level of school completed at |
|
father is Spanish/Hispanic/Latino. Check the |
|
|
the time of delivery) |
|
“No” box if father is not Spanish/Hispanic/Latino) |
|
□ |
8th grade or less |
□ |
No, not Spanish/Hispanic/Latino |
|
□ Yes, Mexican, Mexican American, Chicano |
||||
□ |
9th - 12th grade, no diploma |
|||
□ |
Yes, Puerto Rican |
|||
□ |
High school graduate or GED |
|||
□ |
|
|||
|
completed |
Yes, Cuban |
||
□ |
Some college credit but no degree |
□ |
Yes, other Spanish/Hispanic/Latino |
|
□ Associate degree (e.g., AA, AS) |
|
(Specify)_____________________________ |
||
|
|
|
||
□Bachelor’s degree (e.g., BA, AB, BS)
□Master’s degree (e.g., MA, MS, MEng, MEd, MSW, MBA)
□Doctorate (e.g., PhD, EdD) or Professional degree (e.g., MD, DDS, DVM, LLB, JD)
22.MOTHER’S RACE (Check one or more races to indicate what the mother considers herself to be)
□White
□Black or African American
□American Indian or Alaska Native
(Name of the enrolled or principal tribe)________________
□Asian Indian
□Chinese
□Filipino
□Japanese
□Korean
□Vietnamese
□Other Asian (Specify)______________________________
□Native Hawaiian
□Guamanian or Chamorro
□Samoan
□Other Pacific Islander (Specify)______________________
□Other (Specify)___________________________________
25.FATHER’S RACE (Check one or more races to indicate what the father considers himself to be)
□White
□Black or African American
□American Indian or Alaska Native
(Name of the enrolled or principal tribe)________________
□Asian Indian
□Chinese
□Filipino
□Japanese
□Korean
□Vietnamese
□Other Asian (Specify)______________________________
□Native Hawaiian
□Guamanian or Chamorro
□Samoan
□Other Pacific Islander (Specify)______________________
□Other (Specify)___________________________________
26. PLACE WHERE BIRTH OCCURRED (Check one) |
27. ATTENDANT’S NAME, TITLE, AND NPI |
28. MOTHER TRANSFERRED FOR MATERNAL |
|
□ Hospital |
NAME: _______________________ NPI:_______ |
MEDICAL OR FETAL INDICATIONS FOR |
|
□ Freestanding birthing center |
DELIVERY? □ Yes □ No |
||
|
IF YES, ENTER NAME OF FACILITY MOTHER |
||
□ Home Birth: Planned to deliver at home? 9 Yes 9 No |
TITLE: □ MD □ DO □ CNM/CM □ OTHER MIDWIFE |
||
TRANSFERRED FROM: |
|||
□ Clinic/Doctor’s office |
□ OTHER (Specify)___________________ |
_______________________________________ |
|
□ Other (Specify)_______________________ |
|||
|
REV. 11/2003
|
MOTHER |
29a. DATE OF FIRST PRENATAL CARE VISIT |
|
29b. DATE OF LAST PRENATAL CARE VISIT |
30. TOTAL NUMBER OF PRENATAL VISITS FOR THIS PREGNANCY |
||||||||||||||||||
|
______ /________/ __________ □ No Prenatal Care |
|
|
______ /________/ __________ |
|
|
|
|
|
|
|
|
|||||||||||
|
|
M M |
D D |
|
|
|
YYYY |
|
|
|
M M |
D D |
YYYY |
|
|
_________________________ (If none, enter A0".) |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
31. MOTHER’S HEIGHT |
32. MOTHER’S |
PREPREGNANCY WEIGHT |
33. MOTHER’S WEIGHT |
AT DELIVERY |
34. DID MOTHER GET WIC FOOD FOR HERSELF |
||||||||||||||||
|
|
_______ (feet/inches) |
_________ (pounds) |
|
|
_________ (pounds) |
|
|
DURING THIS PREGNANCY? □ Yes □ No |
||||||||||||||
|
|
35. NUMBER OF PREVIOUS |
36. NUMBER OF OTHER |
37. CIGARETTE SMOKING BEFORE AND DURING PREGNANCY |
|
38. PRINCIPAL SOURCE OF |
|||||||||||||||||
|
|
LIVE BIRTHS (Do not include |
PREGNANCY OUTCOMES |
For each time period, enter either the number of cigarettes or the |
|
PAYMENT FOR THIS |
|||||||||||||||||
|
|
this child) |
|
|
|
|
(spontaneous or induced |
number of packs of cigarettes smoked. IF NONE, ENTER A0". |
|
DELIVERY |
|||||||||||||
|
|
|
|
|
|
|
|
|
losses or ectopic pregnancies) |
Average number of cigarettes or packs of cigarettes smoked per day. |
□ Private Insurance |
||||||||||||
|
|
35a. |
Now Living |
|
35b. Now Dead |
36a. Other Outcomes |
|
||||||||||||||||
|
|
Number _____ |
|
|
Number _____ |
Number _____ |
|
|
|
|
|
|
|
# of cigarettes |
# of packs |
□ Medicaid |
|||||||
|
|
|
|
|
|
|
Three Months Before Pregnancy |
_________ |
|
OR |
________ |
□ |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
First Three Months of Pregnancy |
_________ |
|
OR |
________ |
□ Other |
|||||
|
|
□ None |
|
|
|
□ None |
□ None |
|
|
|
Second Three Months of Pregnancy _________ |
OR |
________ |
||||||||||
|
|
|
|
|
|
|
|
(Specify) _______________ |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Third Trimester of Pregnancy |
_________ |
OR |
________ |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
35c. DATE OF LAST LIVE BIRTH |
36b. DATE OF LAST OTHER |
39. DATE LAST NORMAL MENSES BEGAN |
|
40. MOTHER’S MEDICAL RECORD NUMBER |
|||||||||||||||||
|
|
|
_______/________ |
PREGNANCY OUTCOME |
______ /________/ __________ |
|
|
|
|
|
|
||||||||||||
|
|
|
|
MM |
Y Y Y Y |
_______/________ |
M M |
D D |
YYYY |
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
MM |
Y Y Y Y |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
MEDICAL |
41. RISK FACTORS IN THIS PREGNANCY |
|
43. OBSTETRIC PROCEDURES (Check all that apply) |
46. METHOD OF DELIVERY |
||||||||||||||||||
|
|
|
(Check all that apply) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
AND |
Diabetes |
|
|
|
|
|
|
|
□ Cervical cerclage |
|
|
|
|
|
|
A. Was delivery with forceps attempted but |
||||||
|
HEALTH |
□ |
|
Prepregnancy |
(Diagnosis prior to this pregnancy) |
|
□ Tocolysis |
|
|
|
|
|
|
|
unsuccessful? |
|
|||||||
|
□ |
|
Gestational |
|
(Diagnosis in this pregnancy) |
|
|
External cephalic version: |
|
|
|
|
|
|
□ Yes |
□ No |
|||||||
|
INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. Was delivery with vacuum extraction attempted |
||||||
|
Hypertension |
|
|
|
|
|
|
|
□ Successful |
|
|
|
|
|
|
||||||||
|
|
□ |
|
Prepregnancy |
(Chronic) |
|
|
|
□ Failed |
|
|
|
|
|
|
|
but unsuccessful? |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
□ |
|
Gestational |
(PIH, preeclampsia) |
|
|
□ None of the above |
|
|
|
|
|
|
|
□ Yes |
□ No |
||||||
|
|
□ |
|
Eclampsia |
|
|
|
|
|
|
|
|
|
|
|
C. Fetal presentation at birth |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
□ Previous preterm birth |
|
|
|
|
|
|
|
|
|
|
|
□ |
Cephalic |
|
|||||||
|
|
|
|
44. ONSET OF LABOR (Check all that apply) |
|
|
|
||||||||||||||||
|
|
|
|
|
|
□ |
Breech |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
□ Other previous poor pregnancy outcome (Includes |
|
□ Premature Rupture of the Membranes (prolonged, ∃12 hrs.) |
□ |
Other |
|
|
|||||||||||||||
|
|
perinatal death, |
|
|
|
|
|
|
|
|
|
D. Final route and method of delivery (Check one) |
|||||||||||
|
|
growth restricted birth) |
|
|
□ Precipitous Labor (<3 hrs.) |
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
□ Vaginal/Spontaneous |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
□ Pregnancy resulted from infertility |
|
□ Prolonged Labor (∃ 20 hrs.) |
|
|
|
|
□ Vaginal/Forceps |
||||||||||||||
|
|
check all that apply: |
|
|
|
|
|
|
|
|
|
|
|
□ Vaginal/Vacuum |
|||||||||
|
|
□ |
□ None of the above |
|
|
|
|
|
|
□ Cesarean |
|
||||||||||||
|
|
|
|
Intrauterine insemination |
|
|
|
|
|
|
|
|
|
|
|
|
If cesarean, was a trial of labor attempted? |
||||||
|
|
□ Assisted reproductive technology (e.g., in vitro |
|
|
|
|
|
|
|
|
|
|
|
□ Yes |
|
|
|||||||
|
|
|
45. CHARACTERISTICS OF LABOR AND DELIVERY |
|
|
|
|
|
|||||||||||||||
|
|
|
|
fertilization (IVF), gamete intrafallopian |
|
|
|
|
□ No |
|
|
||||||||||||
|
|
|
|
|
|
|
(Check all that |
apply) |
|
|
|
|
|
|
|
||||||||
|
|
|
|
transfer |
(GIFT)) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
□ |
Induction of labor |
|
|
|
|
|
|
47. MATERNAL MORBIDITY (Check all that apply) |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
□ Mother had a previous cesarean delivery |
|
|
|
|
|
|
|
(Complications associated with labor and |
|||||||||||||
|
|
|
□ |
Augmentation of labor |
|
|
|
|
|
||||||||||||||
|
|
|
|
If yes, how many __________ |
|
|
|
|
|
|
|
delivery) |
|
|
|||||||||
|
|
|
|
|
|
□ |
|
|
|
|
|
□ |
Maternal transfusion |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
□ None of the above |
|
|
□ Steroids (glucocorticoids) for fetal lung maturation |
|
|
□ Third or fourth degree perineal laceration |
|||||||||||||||
|
|
42. INFECTIONS PRESENT AND/OR TREATED |
|
|
received by the mother prior to delivery |
|
|
|
|
□ |
Ruptured uterus |
||||||||||||
|
|
DURING THIS |
PREGNANCY (Check all that apply) |
□ Antibiotics received by the mother during labor |
|
|
□ |
Unplanned hysterectomy |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
□ Clinical chorioamnionitis diagnosed during labor or |
□ Admission to intensive care unit |
|||||||||||
|
|
□ |
Gonorrhea |
|
|
|
|
|
maternal temperature >38°C (100.4°F) |
|
|
□ Unplanned operating room procedure |
|||||||||||
|
|
□ |
Syphilis |
|
|
|
|
|
|
□ Moderate/heavy meconium staining of the amniotic fluid |
|
following delivery |
|||||||||||
|
|
□ |
Chlamydia |
|
|
|
|
□ Fetal intolerance of labor such that one or more of the |
□ None of the above |
||||||||||||||
|
|
□ |
Hepatitis B |
|
|
|
|
|
following actions was taken: |
|
|
|
|
||||||||||
|
|
□ |
Hepatitis C |
|
|
|
|
|
measures, further fetal assessment, or operative delivery |
|
|
|
|
||||||||||
|
|
|
|
|
|
□ Epidural or spinal anesthesia during labor |
|
|
|
|
|
|
|||||||||||
|
|
□ None of the above |
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
□ None of the above |
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NEWBORN
Mother’s Name ________________ |
Mother’s Medical Record No. ____________________ |
NEWBORN INFORMATION
48. NEWBORN MEDICAL RECORD NUMBER |
54. ABNORMAL CONDITIONS OF THE NEWBORN |
55. CONGENITAL ANOMALIES OF THE NEWBORN |
||||||
|
|
|
(Check all that apply) |
□ |
|
(Check all that apply) |
||
49. BIRTHWEIGHT (grams preferred, specify unit) |
□ |
Assisted ventilation required immediately |
Anencephaly |
|
||||
|
□ |
Meningomyelocele/Spina bifida |
||||||
______________________ |
|
following delivery |
□ |
Cyanotic congenital heart disease |
||||
9 grams 9 lb/oz |
□ |
|
|
|
□ |
Congenital diaphragmatic hernia |
||
|
Assisted ventilation required for more than |
|||||||
|
□ |
Omphalocele |
|
|||||
|
|
six hours |
|
|||||
50. OBSTETRIC ESTIMATE OF GESTATION: |
|
□ |
Gastroschisis |
|
||||
|
|
|
|
|
||||
_________________ (completed weeks) |
□ |
NICU admission |
□ |
Limb reduction defect (excluding congenital |
||||
|
|
|
|
|
|
amputation and dwarfing syndromes) |
||
|
□ |
Newborn given surfactant replacement |
□ Cleft Lip with or without Cleft Palate |
|||||
|
□ |
Cleft Palate alone |
|
|||||
|
|
therapy |
|
|||||
51. APGAR SCORE: |
|
|
||||||
|
|
|
|
□ |
Down Syndrome |
|
||
Score at 5 minutes:________________________ |
|
|
|
|
|
|||
□ |
Antibiotics received by the newborn for |
|
□ |
Karyotype confirmed |
||||
If 5 minute score is less than 6, |
|
|||||||
Score at 10 minutes: _______________________ |
|
suspected neonatal sepsis |
□ |
□ |
Karyotype pending |
|||
□ |
Seizure or serious neurologic dysfunction |
Suspected chromosomal disorder |
||||||
|
|
□ |
Karyotype confirmed |
|||||
52. PLURALITY - Single, Twin, Triplet, etc. |
□ Significant birth injury (skeletal fracture(s), peripheral |
□ |
□ |
Karyotype pending |
||||
|
Hypospadias |
|
||||||
(Specify)________________________ |
|
nerve |
injury, and/or soft tissue/solid organ hemorrhage |
|
||||
|
□ |
None of the anomalies listed above |
||||||
|
which |
requires intervention) |
||||||
53. IF NOT SINGLE BIRTH - Born First, Second, |
|
|
|
|
|
|
|
|
Third, etc. (Specify) ________________ |
9 None of the above |
|
|
|
|
|||
|
|
|
|
|
||||
|
|
|
|
|
||||
56. WAS INFANT TRANSFERRED WITHIN 24 HOURS OF DELIVERY? 9 Yes 9 No |
57. IS INFANT LIVING AT TIME OF REPORT? |
58. IS THE INFANT BEING |
||||||
IF YES, NAME OF FACILITY INFANT TRANSFERRED |
|
|
□ Yes □ No □ Infant transferred, status unknown |
BREASTFED AT DISCHARGE? |
||||
TO:______________________________________________________ |
|
|
|
|
□ Yes □ No |
|||
|
|
|
|
|
|
|
|
|
Rev. 11/2003
NOTE: This recommended standard birth certificate is the result of an extensive evaluation process. Information on the process and resulting recommendations as well as plans for future
activities is available on the Internet at: http://www.cdc.gov/nchs/vital_certs_rev.htm.
Documents used along the form
The CDC U.S. Standard Certificate of Live Birth form is essential for registering a birth in the United States. Along with this form, several other documents and forms may be required or beneficial for various purposes, such as obtaining identification, enrolling in school, or accessing healthcare services. Below is a list of commonly used forms and documents that accompany the birth certificate.
- Social Security Card Application (Form SS-5): This form is used to apply for a Social Security number for a newborn. A Social Security number is crucial for tax purposes and accessing government services.
- Certificate of Live Birth (Short Form): Some states provide a shorter version of the birth certificate, which may be sufficient for certain purposes, like enrolling in daycare or school.
- Proof of Residency: Documents such as utility bills or lease agreements may be required to establish residency, especially when applying for government services or educational programs.
- Health Insurance Enrollment Form: This form is necessary to add the newborn to a health insurance plan. Timely enrollment ensures coverage for medical care from birth.
- Immunization Records: These records are vital for enrolling a child in school and keeping track of vaccinations. They may be requested by healthcare providers or educational institutions.
- ADP Pay Stub: This form is crucial for employees as it provides an overview of earnings and deductions, helping them to manage finances effectively. For more information, visit My PDF Forms.
- Application for State Benefits: Some families may need to apply for state assistance programs. This application often requires proof of the child's birth and residency.
- Passport Application: If parents wish to obtain a passport for their newborn, this application will require the birth certificate along with other identification documents.
- School Enrollment Forms: Many educational institutions require specific forms to enroll a child, which may include proof of age and residency, often satisfied by the birth certificate.
These documents are essential for various administrative and legal purposes. Having them prepared and organized can streamline processes related to your child's identity, healthcare, and education.