Download Cna Shower Sheets Template
The CNA Shower Sheets form plays a crucial role in ensuring the health and safety of residents in care facilities. This form is designed for Certified Nursing Assistants (CNAs) to document their observations during a resident's shower, focusing on skin health and any abnormalities that may arise. Key aspects of the form include a visual assessment checklist that covers various skin conditions such as bruising, skin tears, rashes, and lesions. CNAs are instructed to report any abnormalities immediately to the charge nurse, ensuring that any potential issues are addressed promptly. The form also incorporates a body chart for CNAs to accurately describe and graph the location of any skin abnormalities. Additionally, there is a section dedicated to assessing the need for toenail care, further emphasizing the comprehensive approach to resident care. The charge nurse's signature is required to validate the assessment, and any concerns are forwarded to the Director of Nursing (DON) for further review. This structured documentation not only promotes accountability but also enhances communication among the care team, ultimately supporting better health outcomes for residents.
Key takeaways
Filling out and using the CNA Shower Sheets form is an essential process for ensuring the health and safety of residents. Here are seven key takeaways to keep in mind:
- Visual Assessment is Crucial: Conduct a thorough visual assessment of the resident's skin during the shower. This step is vital for identifying any abnormalities.
- Immediate Reporting: If any abnormal skin conditions are observed, report them to the charge nurse immediately. Timely communication can prevent further complications.
- Detailed Documentation: Use the form to document the exact location and description of any abnormalities. Clear documentation helps in tracking the resident's condition over time.
- Body Chart Utilization: Graph all abnormalities on the provided body chart. This visual representation aids in understanding the extent and location of skin issues.
- Toenail Care Assessment: Determine whether the resident needs toenail trimming. This is an important aspect of personal care that can affect overall health.
- Charge Nurse Involvement: The charge nurse must sign the form after their assessment. This adds an extra layer of oversight and ensures that all concerns are addressed.
- Forwarding to DON: If necessary, forward the completed form to the Director of Nursing (DON) for further review. This ensures that any significant issues are escalated appropriately.
Guide to Writing Cna Shower Sheets
Completing the CNA Shower Sheets form requires careful attention to detail. This form is essential for documenting the skin condition of residents after a shower. Following these steps will help ensure that the information is recorded accurately and efficiently.
- Begin by writing the resident's name in the designated space labeled RESIDENT:.
- Next, enter the date of the assessment in the space labeled DATE:.
- Conduct a visual assessment of the resident's skin during the shower. Look for any abnormalities such as bruising, skin tears, or rashes.
- For each abnormality observed, refer to the list provided in the form. Mark the corresponding number next to the description of the abnormality.
- Use the body chart included in the form to indicate the exact location of each abnormality by number.
- After completing the assessment, sign and date the form in the section labeled CNA Signature: and Date:.
- Determine whether the resident needs their toenails cut. Circle Yes or No in the appropriate section.
- Pass the form to the charge nurse for their signature in the section labeled Charge Nurse Signature: and Date:.
- In the Charge Nurse Assessment: section, the charge nurse should provide a brief summary of their evaluation.
- In the Intervention: section, document any actions taken or recommended based on the assessment.
- Finally, indicate whether the report has been forwarded to the Director of Nursing (DON) by circling Yes or No.
- If forwarded, the DON will sign and date the form in the section labeled DON Signature: and Date:.
Browse Other PDFs
Aaa Idp Same Day - Carefully follow all instructions provided on the form to ensure successful processing.
Goodwill Donation Receipt Qr Code - Your support allows us to help those in need.
In order to ensure a smooth and legally binding transaction, it is essential to utilize a proper format like the California Vehicle Purchase Agreement form. This form, which is readily available at TopTemplates.info, helps clarify the agreement between the buyer and seller, detailing important aspects such as sale price, vehicle specifications, and any pertinent warranties.
Texas Temporary Tag - This form is essential for those who need to drive legally while waiting for permanent plates.
Form Preview Example
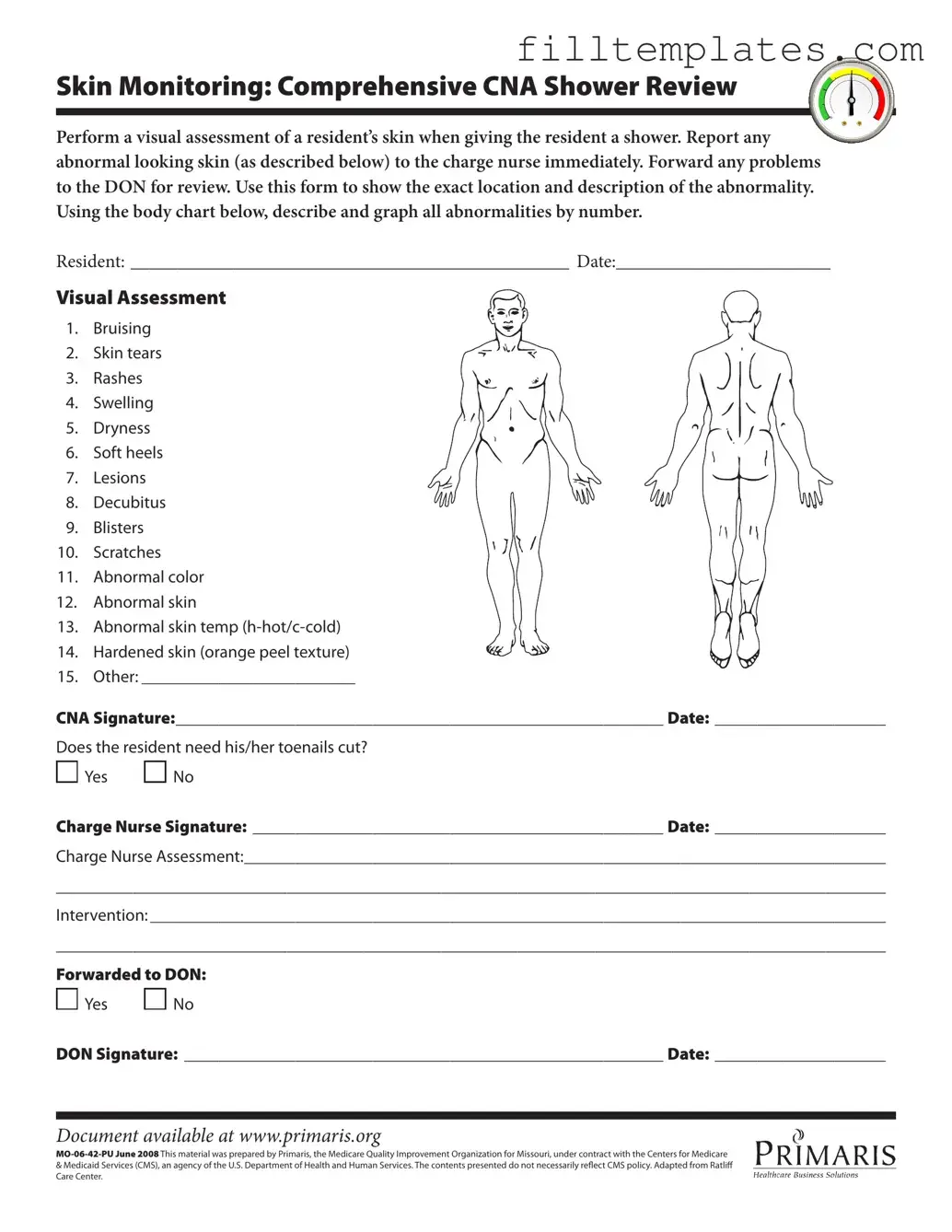
Skin Monitoring: Comprehensive CNA Shower Review
Perform a visual assessment of a resident’s skin when giving the resident a shower. Report any abnormal looking skin (as described below) to the charge nurse immediately. Forward any problems to the DON for review. Use this form to show the exact location and description of the abnormality. Using the body chart below, describe and graph all abnormalities by number.
RESIDENT: _______________________________________________ DATE:_______________________
Visual Assessment
1. Bruising
2. Skin tears
3. Rashes
4. Swelling
5. Dryness
6. Soft heels
7. Lesions
8. Decubitus
9. Blisters
10. Scratches
11. Abnormal color
12. Abnormal skin
13. Abnormal skin temp
14. Hardened skin (orange peel texture)
15. Other: _________________________
CNA Signature:_________________________________________________________ Date: ____________________
Does the resident need his/her toenails cut?

 Yes
Yes 
 No
No
Charge Nurse Signature: ________________________________________________ Date: ____________________
Charge Nurse Assessment:___________________________________________________________________________
_________________________________________________________________________________________________
Intervention: ______________________________________________________________________________________
_________________________________________________________________________________________________
Forwarded to DON:

 Yes
Yes 
 No
No
DON Signature: ________________________________________________________ Date: ____________________
Document available at www.primaris.org
&Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily relect CMS policy. Adapted from Ratlif Care Center.
Documents used along the form
When providing care to residents, several forms and documents are essential for ensuring thorough communication and proper documentation of their needs and conditions. Below is a list of common forms that may accompany the CNA Shower Sheets form. Each document plays a vital role in maintaining the quality of care.
- Care Plan Document: This outlines the individual care needs and goals for each resident. It is developed based on assessments and helps guide daily care activities.
- Incident Report: This form is used to document any unexpected events or accidents involving residents. It ensures that all incidents are recorded and reviewed for safety improvements.
- Skin Assessment Form: This form provides a detailed evaluation of a resident’s skin condition. It helps track changes over time and is essential for identifying potential issues early.
- Medication Administration Record (MAR): This document tracks all medications given to residents. It includes dosages and schedules to ensure proper medication management.
- Vital Signs Record: This form is used to document the resident's vital signs, such as temperature, pulse, and blood pressure. Regular monitoring is crucial for assessing overall health.
- Doctor's Excuse Note: This form is essential for individuals needing verification of their medical-related absences from work or school. It provides legitimacy to the absence while ensuring proper communication between healthcare providers and employers or educational institutions, such as noted in https://smarttemplates.net/fillable-doctors-excuse-note.
- Daily Log: This record captures daily activities, observations, and any significant changes in a resident’s condition. It serves as a comprehensive overview of care provided.
- Referral Form: If a resident requires additional services or specialist consultations, this form facilitates communication between caregivers and external providers.
- Consent for Treatment: This document ensures that residents or their legal representatives agree to specific treatments or procedures. It is essential for legal and ethical compliance.
These documents collectively support the care process and enhance communication among staff members. Proper use of these forms can significantly improve the quality of care provided to residents.