Download Prescription Label Template
The Prescription Label form serves as a vital tool in the medication dispensing process, ensuring that patients receive clear and accurate information about their prescriptions. It typically includes essential details such as the patient's name, medication name, dosage instructions, and the prescribing physician's information. Additionally, the form may provide important warnings or precautions regarding the medication's use, as well as refill information. The layout is designed for easy readability, allowing patients to quickly understand how to take their medication safely and effectively. By standardizing the information presented, the Prescription Label form plays a crucial role in promoting patient safety and adherence to prescribed therapies.
Key takeaways
When filling out and using the Prescription Label form, keep these key takeaways in mind:
- Ensure all patient information is accurate, including name, address, and date of birth.
- Clearly list the medication name, dosage, and instructions for use.
- Include the prescribing physician's information to avoid any confusion.
- Double-check for any allergies or contraindications noted on the form.
- Keep a copy of the completed form for your records and future reference.
- Review the label before dispensing to ensure compliance with regulations.
Following these steps will help ensure that the Prescription Label form is filled out correctly and used effectively.
Guide to Writing Prescription Label
Completing the Prescription Label form accurately is essential for ensuring that medication is dispensed correctly. Follow these steps to fill out the form properly.
- Begin by entering the patient's full name in the designated field. Ensure the spelling is correct to avoid any confusion.
- Next, provide the patient's date of birth. This information helps to confirm the identity of the patient.
- Fill in the medication name as prescribed by the healthcare provider. Use the exact name as it appears on the prescription.
- Indicate the dosage of the medication. This should match the instructions given by the healthcare provider.
- Specify the frequency of dosage. For example, state if the medication is to be taken once a day, twice a day, etc.
- Include the prescribing physician's name. This is important for verification purposes.
- Enter the pharmacy's name and contact information. This ensures that the label can be traced back to the dispensing pharmacy.
- Finally, review all entries for accuracy. Correct any mistakes before finalizing the form.
Browse Other PDFs
Alabama High School Physical Form - Students are encouraged to be honest in their answers, as full disclosure can affect their safety during participation.
To ensure a comprehensive understanding of an individual's qualifications, utilizing a standardized Recommendation Letter form can be highly beneficial; resources such as smarttemplates.net offer templates that simplify the creation of these important documents.
Family Law Financial Affidavit Short Form Florida - The affidavit should reflect the financial situation as of the date of signing.
Form Preview Example
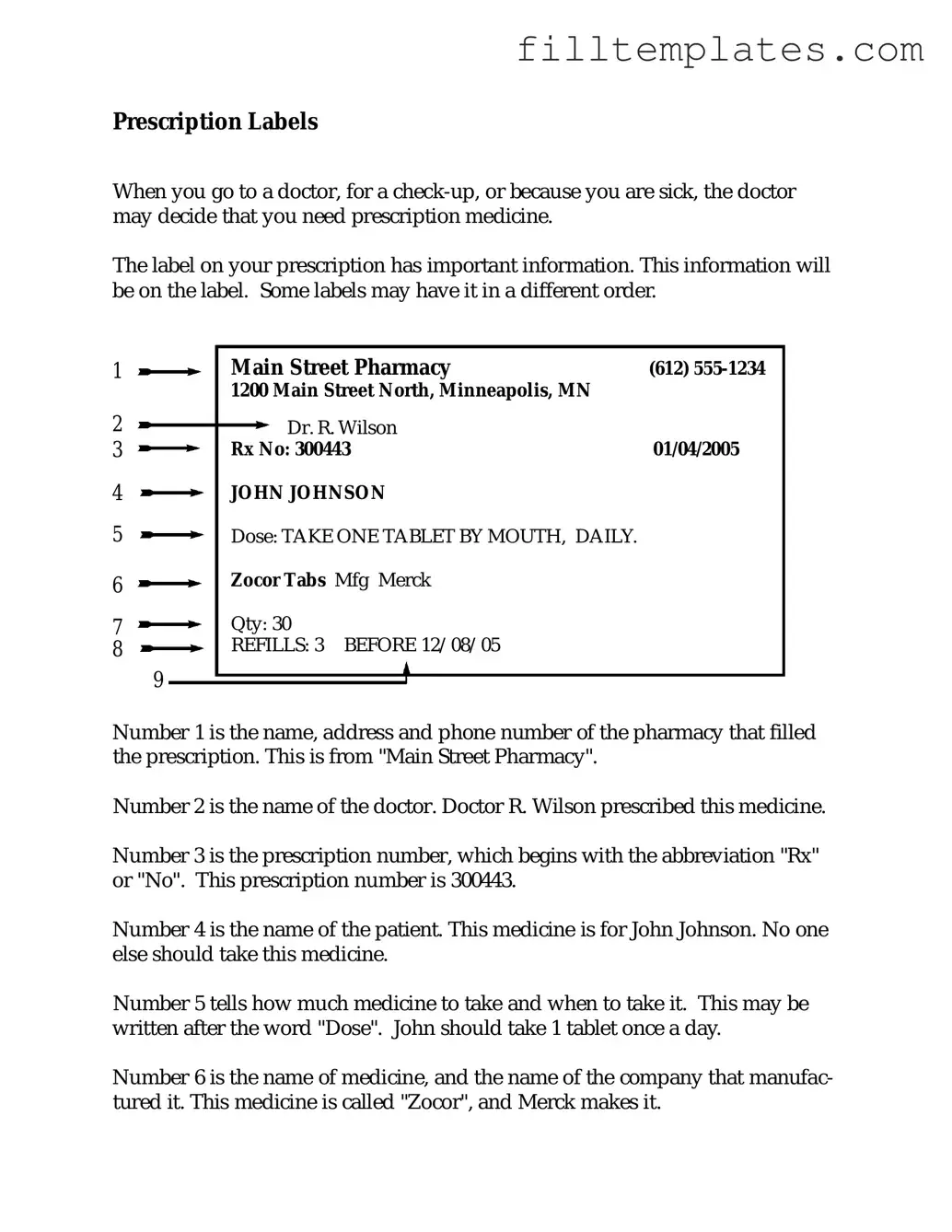
Prescription Labels
When you go to a doctor, for a
The label on your prescription has important information. This information will be on the label. Some labels may have it in a different order.
1 |
|
|
Main Street Pharmacy |
(612) |
|
|
|
|
1200 Main Street North, Minneapolis, MN |
|
|
2 |
|
|
Dr. R. Wilson |
|
|
3 |
|
|
Rx No: 300443 |
01/04/2005 |
|
4 |
|
|
JOHN JOHNSON |
|
|
5 |
|
|
Dose: TAKE ONE TABLET BY MOUTH, DAILY. |
|
|
6 |
|
|
Zocor Tabs Mfg Merck |
|
|
7 |
|
|
Qty: 30 |
|
|
8 |
|
|
REFILLS: 3 BEFORE 12/08/05 |
|
|
|
9 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Number 1 is the name, address and phone number of the pharmacy that filled the prescription. This is from "Main Street Pharmacy".
Number 2 is the name of the doctor. Doctor R. Wilson prescribed this medicine.
Number 3 is the prescription number, which begins with the abbreviation "Rx" or "No". This prescription number is 300443.
Number 4 is the name of the patient. This medicine is for John Johnson. No one else should take this medicine.
Number 5 tells how much medicine to take and when to take it. This may be written after the word "Dose". John should take 1 tablet once a day.
Number 6 is the name of medicine, and the name of the company that manufac- tured it. This medicine is called "Zocor", and Merck makes it.
Number 7 is the number of tablets. This may be written after the abbreviation "Qty" or the word "Quantity". This prescription is for 30 pills.
Number 8 is the number of refills available. When no refills are available the number will be "0".
Number 9 is the expiration date of the prescription. This may be written after "refill before" or the abbreviation "Exp". This is the last date the pharmacy can refill the prescription.
For more information about OTC medicine labels see OTC Labels. For more information about warning labels see Warning Labels.
For more information about the side effects of medicine see Side Effects.
The LaRue Medical Literacy Exercises were created by Charles LaRue through a grant from the Minnesota Department of Education under the supervision of the Minnesota Literacy Council.
©2005 MN Dept of Education
Documents used along the form
When managing prescriptions, several forms and documents complement the Prescription Label form. Each of these documents serves a specific purpose in ensuring proper medication management and patient care. Understanding these documents can enhance communication between healthcare providers and patients.
- Prescription Order Form: This document outlines the specific medication prescribed, including dosage and administration instructions. It serves as the official request from the healthcare provider to the pharmacy.
- Operating Agreement Form: For those establishing their LLC in New York, our detailed operating agreement framework and guidelines provide essential structure for business operations.
- Patient Medication Information Leaflet: This leaflet provides patients with essential information about their medication, including potential side effects, interactions, and proper usage. It is designed to empower patients with knowledge about their treatment.
- Medication Administration Record (MAR): This record tracks when and how medications are administered to patients. It is crucial for healthcare facilities to ensure compliance with treatment protocols and monitor patient responses.
- Prior Authorization Form: Some insurance plans require this form before covering specific medications. It documents the medical necessity of the prescribed treatment, ensuring that patients receive the medications they need.
- Medication Reconciliation Form: This form compares a patient’s current medications against their prescribed medications to prevent errors. It is particularly important during transitions of care, such as hospital admissions or discharges.
- Controlled Substance Prescription Form: For medications classified as controlled substances, this form is necessary to comply with legal regulations. It includes specific information about the patient, prescriber, and medication to ensure proper tracking and accountability.
These documents collectively support the prescription process, ensuring that patients receive safe and effective care. Familiarity with these forms can help patients and providers navigate the complexities of medication management more effectively.