Download Prescription Pad Template
The Prescription Pad form serves as a crucial tool in the healthcare system, streamlining the process of prescribing medication to patients. This form typically includes essential information such as the patient's name, date of birth, and contact details, ensuring that the prescription is accurately tailored to the individual. Additionally, it contains sections for the prescribing physician’s information, including their name, contact number, and medical license number, which helps maintain accountability and traceability. The medication details are prominently displayed, featuring the drug name, dosage, quantity, and instructions for use. Importantly, the form often includes a signature line for the physician, signifying their approval and responsibility for the prescription. Furthermore, many Prescription Pad forms are designed to comply with state regulations, which may vary, thereby ensuring that prescriptions are both valid and legal. Overall, this form is not only a means of communication between healthcare providers and pharmacies but also a vital component in safeguarding patient health and ensuring proper medication management.
Key takeaways
When filling out and using the Prescription Pad form, keep the following key takeaways in mind:
- Ensure all patient information is accurate and up-to-date to avoid any confusion or delays in treatment.
- Clearly specify the medication name, dosage, and instructions to ensure the patient understands how to take the medication.
- Double-check for any potential drug interactions or allergies that the patient may have to prevent adverse effects.
- Keep the completed form secure and confidential, as it contains sensitive patient information.
Guide to Writing Prescription Pad
Completing the Prescription Pad form is an important task that requires attention to detail. This form will help ensure that the necessary information is accurately recorded for the patient’s medication needs. Follow the steps outlined below to fill out the form correctly.
- Begin by writing the patient's full name at the top of the form.
- Next, include the patient's date of birth to help identify them accurately.
- Provide the patient's address, ensuring that it is complete and up to date.
- Indicate the date on which the prescription is being written.
- Clearly write the name of the medication being prescribed.
- Specify the dosage of the medication, including the strength and frequency of administration.
- Include any special instructions for the patient regarding the medication.
- Sign the form with your full name and credentials to validate the prescription.
- Finally, provide your contact information in case the pharmacy needs to reach you for clarification.
Browse Other PDFs
Family Law Financial Affidavit Short Form Florida - The form is an important tool for ensuring fairness in financial matters during divorce or separation.
This essential document serves as a formal agreement and can be beneficial when utilizing a detailed mobile home bill of sale template to ensure a smooth transaction.
Cna Shower Sheet Template - It serves to build trust in the care provided from CNAs to residents.
Form Preview Example
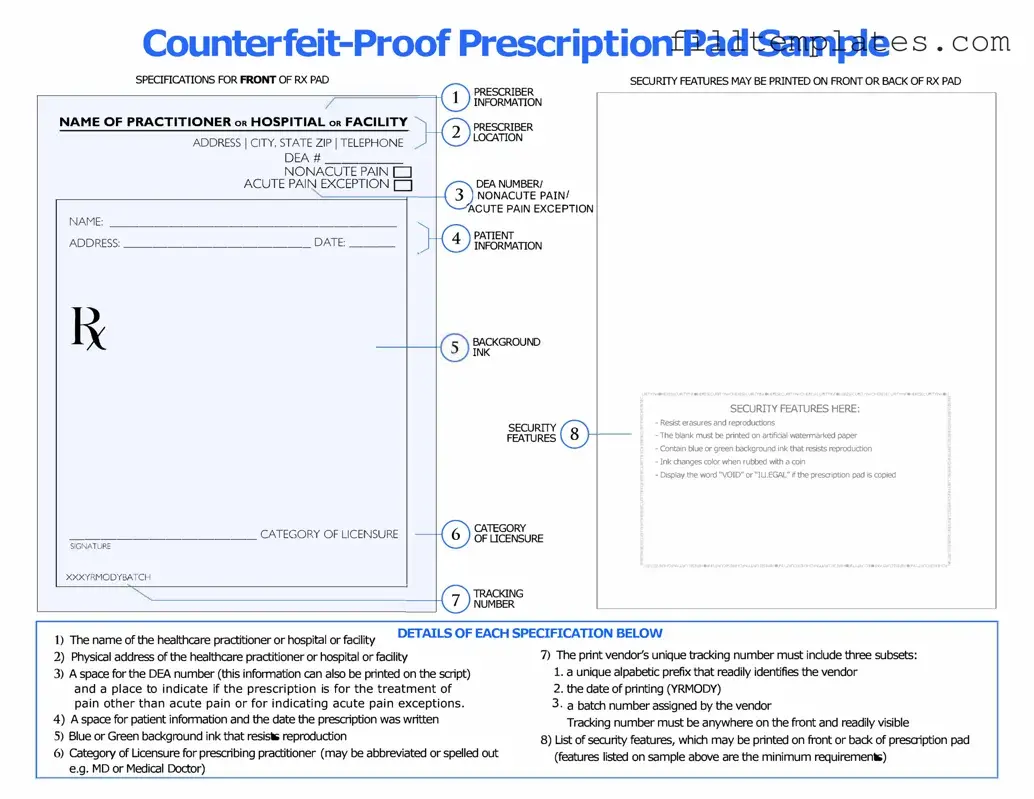
SPECIFICATIONS FOR FRONT OF RX PAD
NAME OF PRACTITIONER oR HOSPITIAL oR FACILITY
ADDRESS I CITY, STATE ZIP I TELEPHONE
DEA# _____□
NONACUTE PAIN
ACUTE PAIN EXCEPTION D
NAME: ___________________
ADDRESS: _____________ DATE: ___
____________ CATEGORY OF LICENSURE
SIGNATURE
XXXYRMODYBATCH
PRESCRIBER
INFORMATION
PRESCRIBER
LOCATION
DEA NUMBER/ NONACUTE PAIN/
ACUTE PAIN EXCEPTION
PATIENT
INFORMATION
BACKGROUND
INK
SECURITY
FEAllJRES
CATEGORY
OF LICENSURE
SECURITY FEAllJRES MAY BE PRINTED ON FRONT OR BACK OF RX PAD
� |
SECURITY FEAllJRES HERE: |
!i, |
|
|
|
|
- Resist erasures and reproductions |
|
|
- The blank must be printed on artificial waterrnarl<ed paper |
|
|
- Contain blue or green background ink that resists reproduction |
|
|
- Ink changes color when rubbed with a coin |
|
|
- Display the word "VOID" or"IU.EGAL" ifthe prescription pad is copied |
� |
|
|
_10HOJNIAl.nn::HS3'd3HOcJNl,Url!nJ=
1) |
The name of the healthc.are practitioner or hospital or facility |
DETAILS OF EACH SPECIFICATION BELOW |
|
|
7) The print vendor's unique tracking number must include three subsets: |
||
2) |
Physic.al address of the healthc.are practitioner or hospital or facility |
||
3) |
A space for the DEA number (this information c.an also be printed on the script) |
1. a unique alpabetic prefix that readily identifies the vendor |
|
|
and a place to indicate if the prescription is for the treatment of |
2. the date of printing (YRMODY) |
|
|
pain other than acute pain or for indicating acute pain exceptions. |
3 • a batch number assigned by the vendor |
|
4) |
A space for patient information and the date the prescription was written |
Tracking number must be anywhere on the front and readily visible |
|
5) |
Blue or Green background ink that resists reproduction |
|
8) List of security features, which may be printed on front or back of prescription pad |
6) |
Category of Licensure for prescribing practitioner (may be abbreviated or spelled out |
(features listed on sample above are the minimum requirements) |
|
|
e.g. MD or Medic.al Doctor) |
|
|
Documents used along the form
When managing prescriptions, healthcare providers often rely on a variety of forms and documents to ensure proper patient care and compliance with regulations. Each of these documents plays a critical role in the overall process of prescribing medications.
- Patient Information Form: This document collects essential details about the patient, including personal information, medical history, and current medications. It helps healthcare providers understand the patient's background and make informed decisions regarding treatment.
- Medication Administration Record (MAR): The MAR is used to track the administration of prescribed medications. It provides a detailed log of when and how medications were given, ensuring that patients receive their treatments as intended and helping to prevent errors.
- Informed Consent Form: Before prescribing certain medications, especially those with significant side effects or risks, healthcare providers often require patients to sign an informed consent form. This document ensures that patients understand the potential benefits and risks associated with their treatment.
- Employment Verification Form: This document is essential for verifying an employee's work history when applying for new positions or loan approvals. For more information, visit OnlineLawDocs.com.
- Refill Authorization Form: When a patient needs a refill for their medication, this form is used to request approval from the prescribing provider. It helps streamline the process and ensures that patients do not run out of necessary medications.
- Drug Utilization Review (DUR) Form: This form is used to evaluate the appropriateness of prescribed medications based on the patient's health history and current medications. It helps identify potential drug interactions and ensures that the prescribed therapy aligns with best practices.
Each of these documents complements the Prescription Pad form, creating a comprehensive framework for safe and effective medication management. By utilizing these forms, healthcare providers can enhance patient safety and improve overall treatment outcomes.