Download SSA SSA-44 Template
The SSA SSA-44 form plays a crucial role in the Social Security Administration's process for individuals seeking to adjust their benefits due to changes in income or financial circumstances. This form is specifically designed for those who wish to request a reduction in their income-related monthly adjustment amount (IRMAA) for Medicare Part B and Part D premiums. By completing the SSA-44, beneficiaries can provide the necessary information to demonstrate that their income has decreased significantly, which may qualify them for lower premium rates. Understanding how to properly fill out this form is essential, as it requires detailed financial information and supporting documentation to substantiate the claim. Timeliness is also important; submitting the SSA-44 promptly can lead to quicker adjustments in premium rates, ensuring that individuals are not overpaying based on outdated income levels. Overall, the SSA SSA-44 form serves as a vital tool for beneficiaries to manage their healthcare costs effectively.
Key takeaways
When dealing with the SSA SSA-44 form, it’s essential to understand its purpose and the implications of filling it out correctly. This form is used to request a reduction in your Social Security benefits based on your current financial situation. Here are some key takeaways to keep in mind:
- Understand the Eligibility Criteria: Before filling out the form, ensure that you meet the eligibility requirements for a reduction in benefits. This typically involves demonstrating financial hardship.
- Gather Necessary Documentation: Collect all required documents that support your request. This may include income statements, proof of expenses, and any other relevant financial information.
- Be Accurate and Honest: Fill out the form with precise information. Providing false information can lead to delays or denial of your request.
- Follow Submission Guidelines: Pay close attention to the instructions regarding how to submit the form. Whether it’s online or via mail, ensure you adhere to the specified guidelines to avoid complications.
- Keep Copies for Your Records: Always retain a copy of the completed form and any supporting documents. This can be invaluable for future reference or in case of any disputes.
By following these key points, you can navigate the SSA SSA-44 form process more effectively, ensuring that your request is handled smoothly and efficiently.
Guide to Writing SSA SSA-44
Filling out the SSA SSA-44 form is a straightforward process that requires careful attention to detail. Once you have completed the form, you will need to submit it to the Social Security Administration for review. Make sure to keep a copy for your records.
- Start by downloading the SSA SSA-44 form from the Social Security Administration's website or obtain a physical copy from your local office.
- Begin filling out your personal information at the top of the form. This includes your name, Social Security number, and address.
- Provide information about your income. Be specific about the sources and amounts. You may need to refer to your financial records.
- Indicate any changes in your circumstances that might affect your benefits. This can include changes in employment, income, or living situation.
- Sign and date the form at the bottom. Your signature confirms that the information provided is accurate to the best of your knowledge.
- Make a copy of the completed form for your records before submitting it.
- Submit the form either by mailing it to the address specified on the form or by visiting your local Social Security office.
Browse Other PDFs
Pest Control Forms Templates - A written notice of thirty days is required for cancellation of the agreement.
Add Money to Netspend Card From Bank Account - Provide the amount, date, and merchant's name for each transaction.
The Employment Verification form is a document used by employers to confirm the employment status of current or former employees. It typically includes information such as job title, dates of employment, and salary details. This form plays a crucial role in various processes, including loan applications and background checks, making it essential for applicants to utilize resources like OnlineLawDocs.com for accurate and efficient completion.
Schedule B (form 941) - The IRS requires this form to verify tax payments made by employers.
Form Preview Example
Form |
Page 1 of 8 |
Discontinue Prior Editions |
|
Social Security Administration |
OMB No. |
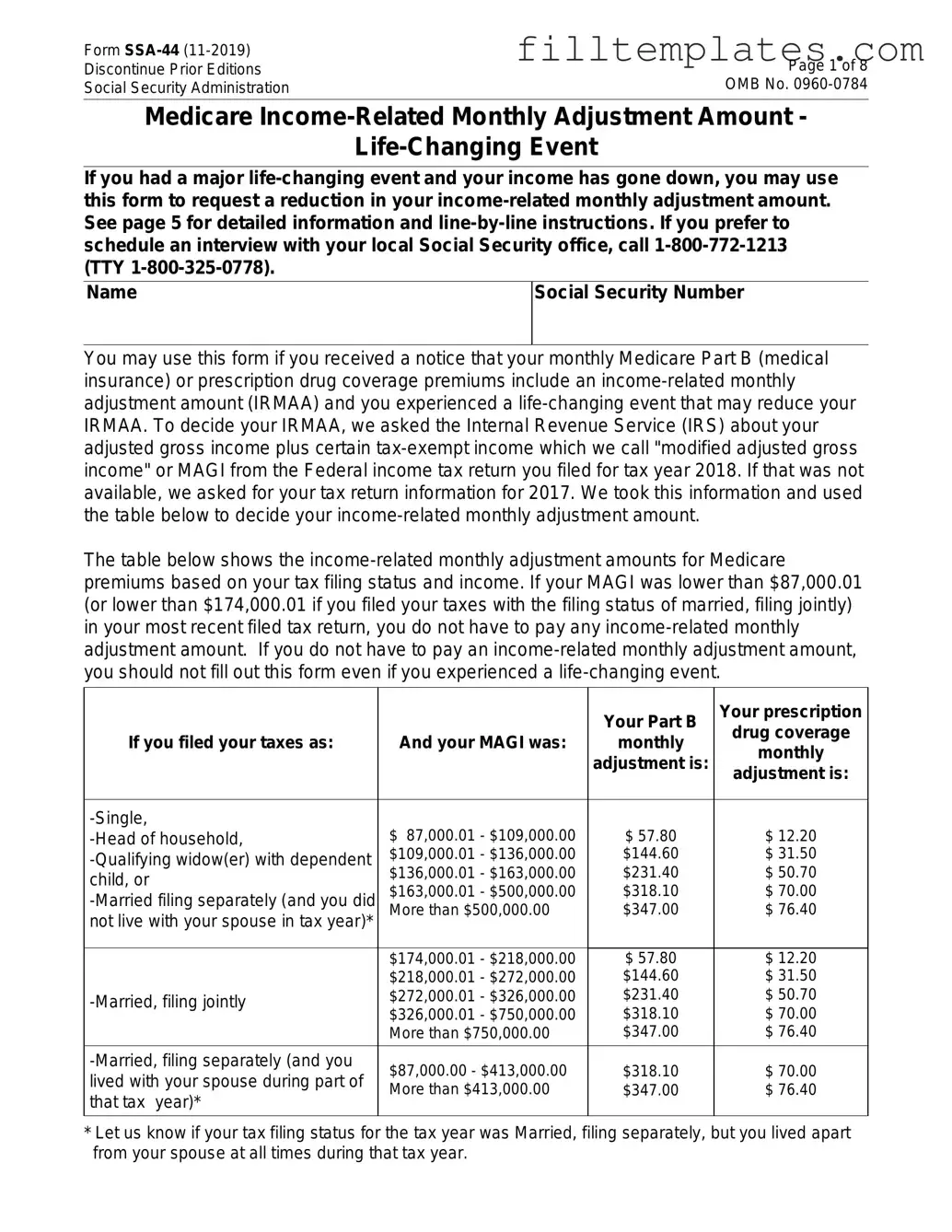
Medicare
If you had a major
Name
Social Security Number
You may use this form if you received a notice that your monthly Medicare Part B (medical insurance) or prescription drug coverage premiums include an
The table below shows the
|
|
Your Part B |
Your prescription |
|
|
|
drug coverage |
||
If you filed your taxes as: |
And your MAGI was: |
monthly |
||
monthly |
||||
|
|
adjustment is: |
||
|
|
adjustment is: |
||
|
|
|
||
|
|
|
|
|
$ 87,000.01 - $109,000.00 |
$ 57.80 |
$ 12.20 |
||
$109,000.01 - $136,000.00 |
$144.60 |
$ 31.50 |
||
child, or |
$136,000.01 - $163,000.00 |
$231.40 |
$ 50.70 |
|
$163,000.01 - $500,000.00 |
$318.10 |
$ 70.00 |
||
More than $500,000.00 |
$347.00 |
$ 76.40 |
||
not live with your spouse in tax year)* |
|
|
|
|
|
|
|
|
|
|
$174,000.01 - $218,000.00 |
$ 57.80 |
$ 12.20 |
|
|
$218,000.01 - $272,000.00 |
$144.60 |
$ 31.50 |
|
$272,000.01 - $326,000.00 |
$231.40 |
$ 50.70 |
||
$326,000.01 - $750,000.00 |
$318.10 |
$ 70.00 |
||
|
||||
|
More than $750,000.00 |
$347.00 |
$ 76.40 |
|
$87,000.00 - $413,000.00 |
$318.10 |
$ 70.00 |
||
lived with your spouse during part of |
||||
More than $413,000.00 |
$347.00 |
$ 76.40 |
||
that tax year)* |
||||
|
|
|
||
|
|
|
|
*Let us know if your tax filing status for the tax year was Married, filing separately, but you lived apart from your spouse at all times during that tax year.
Form |
Page 2 of 8 |
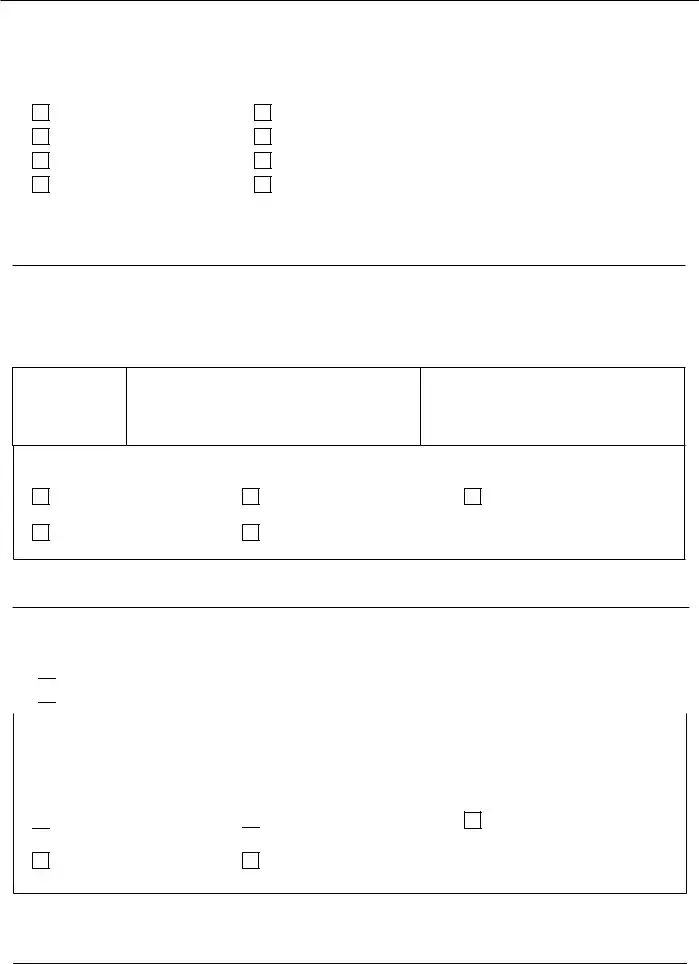
STEP 1: Type of
Check ONE
Marriage |
Work Reduction |
|
Divorce/Annulment |
Loss of |
|
Death of Your Spouse |
Loss of Pension Income |
|
Work Stoppage |
Employer Settlement Payment |
|
Date of |
|
|
|
mm/dd/yyyy |
|
STEP 2: Reduction in Income
Fill in the tax year in which your income was reduced by the
Tax Year
2 0 __ __
Adjusted Gross Income
$ __ __ __ __ __ __ . __ __
$ __ __ __ __ __ __ . __ __
Tax Filing Status for this Tax Year (choose ONE ):
Single |
Head of Household |
Married, Filing Jointly |
Married, Filing Separately |
Qualifying Widow(er) with Dependent Child
STEP 3: Modified Adjusted Gross Income
Will your modified adjusted gross income be lower next year than the year in Step 2?

 No - Skip to STEP 4
No - Skip to STEP 4

 Yes - Complete the blocks below for next year
Yes - Complete the blocks below for next year
Tax Year |
Estimated Adjusted Gross Income |
|
Estimated |
2 0 __ __ |
$ __ __ __ __ __ __. __ __ |
|
$ __ __ __ __ __ __. __ __ |
|
|
|
|
Expected Tax Filing Status for this Tax Year (choose |
ONE ): |
||

 Single
Single
Married, Filing Jointly

 Head of Household
Head of Household
Married, Filing Separately
Qualifying Widow(er) with Dependent Child
Form |
Page 3 of 8 |
STEP 4: Documentation
Provide evidence of your modified adjusted gross income (MAGI) and your
1.Attach the required evidence and we will mail your original documents or certified copies back to you;
OR
2.Show your original documents or certified copies of evidence of your
Note: You must sign in Step 5 and attach all required evidence. Make sure that you provide your current address and a phone number so that we can contact you if we have any questions about your request.
STEP 5: Signature
PLEASE READ THE FOLLOWING INFORMATION CAREFULLY BEFORE SIGNING THIS FORM.
I understand that the Social Security Administration (SSA) will check my statements with records from the Internal Revenue Service to make sure the determination is correct.
I declare under penalty of perjury that I have examined the information on this form and it is true and correct to the best of my knowledge.
I understand that signing this form does not constitute a request for SSA to use more recent tax year information unless it is accompanied by:
•Evidence that I have had the
•A copy of my Federal tax return; or
•Other evidence of the more recent tax year's modified adjusted gross income.
Signature
Phone Number
Mailing Address
Apartment Number
City
State
ZIP Code
Form |
Page 4 of 8 |
|
|
THE PRIVACY ACT
We are required by sections 1839(i) and
We rarely use the information you supply for any purpose other than for determining a potential reduction in IRMAA. However, the law sometimes requires us to give out the facts on this form without your consent. We may release this information to another Federal, State, or local government agency to assist us in determining your eligibility for a reduction in your IRMAA, if Federal law requires that we do so, or to do the research and audits needed to administer or improve our efforts for the Medicare program.
We may also use the information you provide in computer matching programs. Matching programs compare our records with records kept by other Federal, state or local government agencies. We will also compare the information you give us to your tax return records maintained by the IRS. The law allows us to do this even if you do not agree to it. Information from these matching programs can be used to establish or verify a person’s eligibility for Federally funded or administered benefit programs and for repayment of payments or delinquent debts under these programs.
Explanations about these and other reasons why information you provide us may be used or given out are available in Systems of Records Notice
Paperwork Reduction Act Statement - This information collection meets the requirements of 44 U.S.C. § 3507, as amended by section 2 of the Paperwork Reduction Act of 1995. You do not need to answer these questions unless we display a valid Office of Management and Budget control number. We estimate that it will take about 45 minutes to read the instructions, gather the facts, and answer the questions. SEND OR BRING THE COMPLETED FORM TO
YOUR LOCAL SOCIAL SECURITY OFFICE. The office is listed under U. S. Government agencies in your telephone directory or you may call Social Security at
Form |
Page 5 of 8 |
INSTRUCTIONS FOR COMPLETING FORM
Medicare
You do not have to complete this form in order to ask that we use your information about your modified adjusted gross income for a more recent tax year. If you prefer, you may call
Identifying Information
Print your full name and your own Social Security Number as they appear on your Social Security card. Your Social Security Number may be different from the number on your Medicare card.
STEP 1
You should choose only one
|
Use this category if... |
|
|
|
Marriage |
You entered into a legal marriage. |
|
|
|
|
|
|
Divorce/Annulment |
Your legal marriage ended, and you will not file a joint return |
|
|
with your spouse for the year. |
|
|
|
|
|
|
|
Death of Your Spouse |
Your spouse died. |
|
|
|
|
|
|
Work Stoppage or Reduction |
You or your spouse stopped working or reduced the hours |
|
|
that you work. |
|
|
|
|
|
|
|
|
You or your spouse experienced a loss of |
|
|
|
property that was not at your direction (e.g., not due to the |
|
|
Loss of |
sale or transfer of the property). This includes loss of real |
|
|
property in a Presidentially or |
|
|
|
Property |
|
|
|
disaster area, destruction of livestock or crops due to natural |
|
|
|
|
|
|
|
|
disaster or disease, or loss of property due to arson, or loss |
|
|
|
of investment property due to fraud or theft. |
|
|
|
|
|
|
Loss of Pension Income |
You or your spouse experienced a scheduled cessation, |
|
|
termination, or reorganization of an employer's pension plan. |
|
|
|
|
|
|
|
|
You or your spouse receive a settlement from an employer |
|
|
Employer Settlement Payment |
or former employer because of the employer's bankruptcy or |
|
|
|
reorganization. |
|
|
|
|
|

Form |
Page 6 of 8 |
INSTRUCTIONS FOR COMPLETING FORM
STEP 2
Supply information about the more recent year's modified adjusted gross income (MAGI). Note that this year must reflect a reduction in your income due to the
Tax Year
•Fill in both empty spaces in the box that says “20_ _". The year you choose must be more recent than the year of the tax return information we used. The letter that we sent you tells you what tax year we used.
•
•
•
Choose this year (the "premium year") - if your modified adjusted gross income is lower this year than last year. For example, if you request that we adjust your
1.Your income was not reduced until 2020; or
2.Your income was reduced in 2019, but will be lower in 2020.
Choose last year (the year before the "premium year," which is the year for which you want us to adjust your IRMAA) - if your MAGI is not lower this year than last year. For example, if you request that we adjust your 2020
Exception: If we used IRS information about your MAGI 3 years before the premium year, you may ask us to use information from 2 years before the premium year. For example, if we used your income tax return for 2017 to decide your 2020 IRMAA, you can ask us to use your 2018 information.
• If you have any questions about what year you should use, you should call SSA.
Adjusted Gross Income
•Fill in your actual or estimated adjusted gross income for the year you wrote in the “tax year” box. Adjusted gross income is the amount on line 7 of IRS form 1040. If you are providing an estimate, your estimate should be what you expect to enter on your tax return for that year.
•Fill in your actual or estimated
Filing Status
•Check the box in front of your actual or expected tax filing status for the year you wrote in the “tax year” box.

Form |
Page 7 of 8 |
INSTRUCTIONS FOR COMPLETING FORM
STEP 3
Complete this step only if you expect that your MAGI for next year will be even lower and will reduce your IRMAA below what you told us in Step 2 using the table on page 1. We will record this information and use it next year to determine your Medicare
Tax Year
•Fill in both empty spaces in the box that says “20 _ _ ” with the year following the year you wrote in Step 2. For example, if you wrote "2020" in Step 2, then write "2021" in Step 3.
Adjusted Gross Income
•Fill in your estimated adjusted gross income for the year you wrote in the “tax year” box. Adjusted gross income is the amount you expect to enter on line 7 of IRS form 1040 when you file your tax return for that year.
•Fill in your estimated
Filing Status
•Check the box in front of your expected tax filing status for the year you wrote in the “tax year” box.
STEP 4
Provide your required evidence of your MAGI and your
Modified Adjusted Gross Income Evidence
If you have filed your Federal income tax return for the year you wrote in Step 2, then you must provide us with your signed copy of your tax return or a transcript from IRS. If you provided an estimate in Step 2, you must show us a signed copy of your tax return when you file your Federal income tax return for that year.
We must see original documents or certified copies of evidence that the

Form |
Page 8 of 8 |
|
|
|
|
Evidence |
||
|
|
|
Marriage |
An original marriage certificate; or a certified copy of a public record of |
|
marriage. |
||
|
||
Divorce/Annulment |
A certified copy of the decree of divorce or annulment. |
|
|
|
|
Death of Your Spouse |
A certified copy of a death certificate, certified copy of the public record of |
|
death, or a certified copy of a coroner’s certificate. |
||
|
An original signed statement from your employer; copies of pay stubs; |
|
Work Stoppage or |
original or certified documents that show a transfer of your business. |
|
Note: In the absence of such proof, we will accept your signed statement, |
||
Reduction |
||
|
under penalty of perjury, on this form, that you partially or fully stopped |
|
|
working or accepted a job with reduced compensation. |
|
|
|
|
|
An original copy of an insurance company adjuster’s statement of loss or a |
|
Loss of Income- |
letter from a State or Federal government about the uncompensated loss. If |
|
the loss was due to investment fraud (theft), we also require proof of |
||
Producing Property |
||
conviction for the theft, such as a court document citing theft or fraud |
||
|
||
|
relating to you or your spouse's loss. |
|
|
|
|
Loss of Pension |
A letter or statement from your pension fund administrator that explains the |
|
Income |
reduction or termination of your benefits. |
|
|
|
|
Employer Settlement |
A letter from the employer stating the settlement terms of the bankruptcy |
|
Payment |
court and how it affects you or your spouse. |
|
|
|
|
STEP 5 |
|
Read the information above the signature line, and sign the form. Fill in your phone number and current mailing address. It is very important that we have this information so that we can contact you if we have any questions about your request.
Important Facts
•When we use your estimated MAGI information to make a decision about your
•If you provide an estimate of your MAGI rather than a copy of your Federal tax return, we will ask you to provide a copy of your tax return when you file your taxes.
•If your estimate of your MAGI changes, or you amend your tax return for that reason, you will need to contact us to update our records. If you do not contact us, we may have to make corrections later including retroactive assessments or refunds.
•We will use your estimate provided in Step 2 to make a decision about the amount of your
•IRS sends us your tax return information for the year used in Step 2; or
•You provide a signed copy of your filed Federal income tax return or amended Federal income tax return with a different amount; or
•You provide an updated estimate.
•If we used information from IRS about a tax year when your filing status was Married filing separately, but you lived apart from your spouse at all times during that year, you should contact us at
Documents used along the form
The SSA SSA-44 form, known as the "Request for Reconsideration," is a crucial document used by individuals seeking to appeal a decision made by the Social Security Administration regarding their benefits. When completing this process, several other forms and documents may also be necessary to support your claim or appeal. Below is a list of commonly used forms and documents that accompany the SSA SSA-44.
- SSA-16: This is the "Application for Disability Insurance Benefits." Individuals use this form to apply for Social Security Disability Insurance (SSDI) benefits. It gathers essential information about the applicant's work history and medical condition.
- SSA-827: The "Authorization to Disclose Information to the Social Security Administration" form allows the SSA to obtain medical records and other information from healthcare providers. This form is vital for establishing the medical basis of a disability claim.
- SSA-3368: This is the "Disability Report – Adult." It collects detailed information about an individual's medical conditions, treatments, and limitations. This report is often required when applying for SSDI or appealing a denial.
- SSA-3373: Known as the "Function Report – Adult," this form asks applicants to describe how their disability affects their daily activities. It provides the SSA with insight into the functional limitations experienced by the individual.
- New York ATV Bill of Sale Form: When transferring ownership of an All-Terrain Vehicle, refer to our essential New York ATV Bill of Sale documentation guide to ensure all legal requirements are met.
- SSA-45: The "Request for Reconsideration" form is used when an individual wishes to appeal a decision regarding their Social Security benefits. This form is essential for initiating the reconsideration process.
- SSA-3441: This is the "Disability Update Report." It is used to provide updated information about a claimant's medical condition and work status. This report is often required for ongoing eligibility reviews.
- SSA-561: The "Request for Reconsideration" form is specifically for appealing decisions related to Supplemental Security Income (SSI) claims. It serves a similar purpose to the SSA-44 but focuses on SSI benefits.
Understanding these forms and documents is essential for anyone navigating the Social Security appeals process. Each plays a specific role in ensuring that your case is thoroughly reviewed and that all relevant information is considered. Preparing these documents accurately can significantly impact the outcome of your appeal.